Tips to improve the Aging Process for the Female Athlete
What is the definition of INSANITY for the aging athlete?
Doing the same fueling and training program over and over again expecting different results.
What am I learning from Dr. Stacy Sims and her Menopause 2.0 online course?
Traditional methods that we are used to following as the long slow distance for endurance athletes…these are not adequate for improving BONE, MUSCLE, or BODY COMPOSITION.
I get it… I am experiencing loss of power, strength, speed, body composition and joint tightness.
Menopause 2.0 Notes:
The other aspect we have to remember is when we don’t have those estrogen receptors working for us, and estrogen is not as strong a stimulus, then we also have a reduction in the body’s ability to regenerate the cells. So instead of going, hey, it’s damaged, let’s fix it, we have an increase in that cell death instead of an increase in regeneration and helping those cells survive.
Now, when we look at what’s happening above board here with the signaling to kill off more cells and generate more oxidation, then we have a secondary aspect with regards to how the body’s responding to this kind of tissue breakdown.
When we have an increased amount of breakdown, it requires more fuel to be able to accommodate for the enzymes and the responses that are needed to help clean this up.
When we have this stuff going on, then we also look and see, hey, when we are having that decrease in progesterone and we have a decrease in insulin sensitivity, it is primarily an impairment in our insulin signaling.
When we have an impairment in insulin signaling, then we have a reduction in the body’s ability to have a muscle contraction, to uptake more glucose, because if you’re looking here at the integral parts of muscle, we are having the signaling not to regenerate and repair that might be damaged from oxidation because of the increased oxidative stress within the mitochondria.
If you’re having damage to the cells, then you’re not going to get a really strong contraction, and you’re also not going to get the ability for your body to pull glucose in through a muscle contraction.
The aspect of insulin working to help pull this in is another factor where your body’s like, I can’t handle that signaling.
This is how we get more of that insulin resistance. In the fact that we can’t actually pull that glucose in, but we still need fuel to take care of all of these things that are going on within the muscle cell, we have a signal to increase our lipid accumulation primarily because lipids are a key factor for our cell membrane.
In addition to all of these factors that are breaking down and the signaling that’s going on, we have an increased amount of inflammation because inflammation is a way of your body trying to preserve and help tissue, either from a molecular structure all the way up to whole body organs.
This is what’s happening from that molecular aspect of why now we feel like we are puffy and we are not able to generate strength, we’re not very powerful, we are tending to put on more fat mass and losing our lean mass.
I want to get a little bit more into the muscle contraction aspect, and the estrogen receptors that are actually in that process of a muscle contraction, ’cause it’s gonna be very important for you to understand why we need to change our resistance training to lift heavy.
This is a nerve that’s coming down to stimulate a muscle fiber. So how does this nerve stimulate the muscle fiber?
We have this thing right here called a gap junction. So if we look in here, we see that we have little vesicles in here.
These are the holding pattern really for acetylcholine. Now acetylcholine is a neurotransmitter, and that acetylcholine will be pushed out of the end of the nerve cell, the end of the nerve, to then come down and stimulate these receptors that are on that muscle fiber.
ChatGPT
As of my last update in September 2021, Dr. Stacy Sims is a well-known exercise physiologist and nutrition scientist, who has conducted extensive research on the impact of hormones, including estrogen, on female athletes’ performance. While I can’t provide information on her latest research beyond that date, I can discuss the general knowledge up to that point.
Estrogen is a hormone that plays a crucial role in the female body, affecting various physiological processes. In the context of athletic performance, lower estrogen levels can have several potential impacts:
- Muscle Strength: Estrogen is believed to have a positive effect on muscle strength. When estrogen levels are lower, women may experience a reduction in muscle strength compared to when their estrogen levels are higher.
- Muscle Power: Lower estrogen levels may also lead to a decrease in muscle power output. Power is the combination of strength and speed, so reductions in both factors can contribute to a decline in power performance.
- Tendon and Ligament Health: Estrogen also plays a role in maintaining the health and integrity of tendons and ligaments. Reduced estrogen levels may increase the risk of injury to these connective tissues.
- Recovery: Estrogen can influence the rate of muscle recovery after exercise. Lower estrogen levels might lead to slower recovery times, impacting an athlete’s ability to perform optimally in subsequent training sessions or competitions.
It is essential to note that the impact of estrogen on performance can vary among individuals, and it depends on the specific sport, training regimen, and genetic factors. Additionally, other hormones, such as progesterone, also play a role in the female body and can interact with estrogen to influence performance outcomes.
Dr. Stacy Sims’ research aims to understand these hormonal interactions better and how they can be optimized to enhance performance and training strategies for female athletes. As research in this field is continually evolving, I recommend checking more recent sources or Dr. Stacy Sims’ publications and interviews to get the most up-to-date and comprehensive information on this topic.

What causes female athlete to feel puffy, inflamed, lack of power and lack of strength?
- Menstrual Cycle and Hormonal Changes: Female athletes’ hormonal fluctuations during the menstrual cycle can affect their performance. Changes in estrogen and progesterone levels may lead to water retention, bloating, and perceived puffiness. Additionally, hormonal variations can impact energy levels, power output, and strength during different phases of the cycle.
- Overtraining or Poor Recovery: Excessive training without adequate recovery can lead to overtraining syndrome, causing inflammation, fatigue, and decreased performance. Proper rest, nutrition, and sufficient sleep are crucial for athletes to perform at their best.
- Inadequate Nutrition: Insufficient calorie intake or nutrient deficiencies can result in reduced muscle power and strength. Proper nutrition, including adequate protein intake, is essential for muscle repair and growth.
- Dehydration: Lack of proper hydration can lead to reduced blood volume and decreased power and strength performance.
- Injury or Overuse: Injuries or overuse of certain muscle groups can cause localized inflammation and impair strength and power in those areas.
- Chronic Inflammatory Conditions: Some athletes may suffer from chronic inflammatory conditions, such as autoimmune disorders or chronic overtraining, which can lead to a persistent feeling of puffiness and reduced performance.
- Sleep Deprivation: Inadequate sleep can negatively impact hormone levels, recovery, and overall athletic performance.
- Stress: Chronic stress can lead to hormonal imbalances and impact an athlete’s physical and mental well-being, affecting performance.
- Medical Conditions: Certain medical conditions, like thyroid disorders or anemia, can cause fatigue, weakness, and reduced athletic performance.
- Training Program or Technique: Inappropriate training programs or incorrect exercise techniques can lead to injuries, inflammation, and decreased strength and power.
It is essential for female athletes experiencing these symptoms to consult with a healthcare professional, sports nutritionist, or a qualified coach. Identifying the underlying causes and making appropriate adjustments to training, nutrition, and lifestyle can help improve performance and overall well-being. Every athlete’s situation is unique, so personalized assessments and solutions are vital for optimal performance.
How to females become more insulin resistance as we age?

- Hormonal Changes: During perimenopause and menopause, there is a decline in estrogen levels. Estrogen plays a role in promoting insulin sensitivity, so its reduction can contribute to insulin resistance. Additionally, hormonal fluctuations during the menstrual cycle can also impact insulin sensitivity at different times of the month.
- Decreased Physical Activity: As people age, they may become less physically active, leading to decreased muscle mass and reduced insulin sensitivity. Regular exercise helps improve insulin sensitivity and glucose regulation.
- Changes in Body Composition: Aging is often associated with a shift in body composition, including increased fat mass and decreased muscle mass. Higher levels of body fat, especially visceral fat (fat around the organs), are linked to insulin resistance.
- Dietary Habits: Unhealthy eating patterns, such as consuming excessive refined carbohydrates, added sugars, and processed foods, can contribute to insulin resistance over time.
- Weight Gain: With age, many people tend to gain weight, which can worsen insulin resistance. Excess weight, particularly around the abdomen, is strongly associated with insulin resistance.
- Genetics: Some individuals may have a genetic predisposition to insulin resistance, making them more susceptible to developing this condition as they age.
- Sleep Issues: Sleep disturbances become more common with age, and poor sleep quality or insufficient sleep can negatively impact insulin sensitivity.
- Stress: Chronic stress can lead to hormonal imbalances and contribute to insulin resistance.
- Sedentary Lifestyle: A decrease in overall physical activity and prolonged periods of sitting or inactivity can contribute to insulin resistance.
It is essential to note that not all females will experience increased insulin resistance as they age, and individual factors can vary.
To help prevent or manage insulin resistance, lifestyle modifications play a crucial role:
- Engage in regular physical activity, including both aerobic exercises and strength training.
- Follow a balanced and nutritious diet, focusing on whole foods, vegetables, lean proteins, and healthy fats.
- Maintain a healthy weight and body composition.
- Get enough quality sleep each night.
- Manage stress through relaxation techniques, mindfulness, and other stress-reduction strategies.
How is the adrenal gland involved in our hormone production?
- Adrenal Cortex: The outer layer of the adrenal gland, known as the adrenal cortex, is responsible for producing corticosteroid hormones. These hormones can be further divided into three main types:a. Glucocorticoids: The primary glucocorticoid produced is cortisol. Cortisol plays a key role in the body’s stress response, helping to regulate metabolism, blood sugar levels, and the immune system. It also helps the body respond to stress by increasing glucose availability for energy.b. Mineralocorticoids: The main mineralocorticoid produced is aldosterone. Aldosterone is involved in the regulation of blood pressure and electrolyte balance, particularly sodium and potassium levels, by acting on the kidneys.
c. Androgens: The adrenal cortex also produces small amounts of male sex hormones called androgens, such as dehydroepiandrosterone (DHEA). While androgens are produced in smaller quantities compared to the gonads (testes in males and ovaries in females), they can have various effects on the body, including contributing to the female sex hormone production.
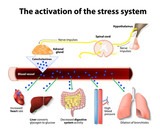
- Adrenal Medulla: The inner portion of the adrenal gland is known as the adrenal medulla. It is part of the sympathetic nervous system and plays a role in the body’s immediate stress response, often referred to as the “fight or flight” response. The adrenal medulla secretes two main hormones:a. Epinephrine (Adrenaline): This hormone is released rapidly in response to stress or danger. It increases heart rate, blood pressure, and the supply of oxygen and glucose to the brain and muscles, preparing the body for immediate action.b. Norepinephrine (Noradrenaline): Norepinephrine has similar effects to adrenaline but acts more on blood vessel constriction, increasing blood pressure.
Together, the hormones produced by the adrenal glands play a crucial role in the body’s stress response, metabolism, immune function, blood pressure regulation, and electrolyte balance.
Any dysregulation or dysfunction of the adrenal glands can lead to various health issues and hormone-related disorders. For example, conditions like Cushing’s syndrome (excess cortisol) or Addison’s disease (insufficient cortisol and aldosterone) are caused by problems with the adrenal glands and their hormone production.
After menopause, the ovaries significantly reduce their production of sex hormones, primarily estrogen and progesterone. However, other sources of sex hormones remain in the body, including the adrenal glands.
The adrenal glands are small endocrine glands located on top of each kidney. They produce several hormones, including cortisol (a stress hormone), aldosterone (a hormone involved in regulating salt and water balance), and small amounts of androgens (male sex hormones). These androgens include dehydroepiandrosterone (DHEA) and androstenedione.
Post menopause, when the ovaries are no longer producing significant amounts of estrogen and progesterone, the adrenal glands become a more important source of androgens. These androgens can be converted into estrogens in peripheral tissues, such as fat cells, through a process called aromatization.
The conversion of androgens into estrogens in peripheral tissues helps to maintain some estrogen levels in the body after menopause. While the levels of estrogens produced this way are much lower than what the ovaries produce before menopause, they can still contribute to various physiological processes that are influenced by estrogen, such as bone health and cardiovascular health.
The balance between androgens and estrogens in postmenopausal women can vary among individuals and may be influenced by factors such as genetics and overall health. Moreover, some women may experience symptoms related to hormonal changes after menopause, and the contribution of adrenal androgens to hormone levels may play a role in those symptoms.
It’s important to note that the adrenal glands’ role in sex hormone production post menopause is secondary to the ovaries’ role before menopause.
How does estrogen related to inflammation?
ChatGPT
- Pro-Inflammatory Effects: Estrogen can promote inflammation in certain situations. For example:
- Immune Response: Estrogen can stimulate the immune system and increase the production of certain inflammatory molecules, such as cytokines and chemokines. This effect is particularly evident during the menstrual cycle when estrogen levels fluctuate, leading to changes in immune responses.
- Injury and Tissue Damage: After tissue injury or damage, estrogen can enhance the inflammatory response, promoting the recruitment of immune cells to the affected area for tissue repair.
- Autoimmune Diseases: In some autoimmune conditions, such as systemic lupus erythematosus (SLE), estrogen may exacerbate inflammation by stimulating the immune system and contributing to disease progression.
- Anti-Inflammatory Effects: On the other hand, estrogen can also exhibit anti-inflammatory properties:
- Immune Modulation: In certain contexts, estrogen can suppress inflammatory responses and modulate the immune system. It may downregulate the production of some pro-inflammatory molecules, helping to maintain immune balance.
- Neuroprotective Effects: Estrogen is believed to have neuroprotective effects, reducing inflammation in the brain and potentially mitigating the effects of neurodegenerative diseases.
- Cardiovascular Health: Estrogen has been shown to have vasodilatory and anti-inflammatory effects on blood vessels, which can contribute to cardiovascular health.
The effects of estrogen on inflammation can also be influenced by other factors, such as age, genetics, and the presence of other hormones. For example, during menopause, when estrogen levels decline, women may experience changes in their inflammatory responses.
Does insulin or glucose enter the muscle cells for energy?
When we eat food, especially carbohydrates, the body breaks down the carbohydrates into glucose, which enters the bloodstream. As blood glucose levels rise, the pancreas releases insulin into the bloodstream. Insulin then acts as a “key” to unlock the cell membranes of various tissues, allowing glucose to enter the cells and be used as a source of energy.
In muscle cells, glucose is taken up from the bloodstream and used for energy production through a process called glycolysis. During glycolysis, glucose is broken down to produce ATP (adenosine triphosphate), the body’s primary energy currency. ATP is then utilized for muscle contraction and various other cellular processes that require energy.
Insulin’s role is to facilitate the transport of glucose into the cells and help regulate blood glucose levels. When insulin is functioning correctly, it promotes the uptake of glucose into muscle cells, liver cells, and fat cells, keeping blood glucose levels within a healthy range.
In contrast, insulin itself does not enter the cells to provide energy. Its primary function is to regulate glucose metabolism and maintain glucose homeostasis in the body.
Why and how do female athletes have a hormonal shift decreasing fat metabolism?
During menopause, there are significant fluctuations in estrogen and progesterone levels. These hormonal changes can impact fat metabolism in the following ways:
- Increased Fat Storage: With declining estrogen levels, there is a tendency for increased fat storage, especially in the abdominal region. This shift is commonly referred to as central or abdominal adiposity. Estrogen plays a role in regulating fat distribution, and reduced estrogen levels may lead to a shift in fat deposition from subcutaneous (under the skin) to visceral (around organs) fat.
- Slower Metabolic Rate: As women age and their lean muscle mass naturally decreases (a process called sarcopenia), their metabolic rate may slow down. A lower metabolic rate means the body burns fewer calories at rest, which can contribute to weight gain or difficulty in maintaining weight.
- Reduced Fat Oxidation: Estrogen is believed to play a role in enhancing fat oxidation, the process by which the body breaks down fats for energy. With declining estrogen levels, there may be a reduction in the body’s ability to efficiently utilize fat as a fuel source during exercise.
- Insulin Sensitivity Changes: During menopause, some women may experience reduced insulin sensitivity, which can impact how the body processes and stores carbohydrates and fats. Reduced insulin sensitivity may lead to increased fat storage and difficulties in managing blood sugar levels.
It’s essential to note that the effects of menopause on fat metabolism can vary among individuals and depend on factors such as genetics, lifestyle, and overall health. While hormonal changes play a significant role, other factors, such as diet, physical activity, and stress, also influence body composition and metabolism.
For aging female athletes, addressing these changes through a combination of regular exercise, strength training, a balanced diet, and lifestyle modifications can help support healthy fat metabolism and overall well-being. Working with healthcare professionals, such as sports physicians, dietitians, and endocrinologists, can provide tailored guidance to optimize performance and mitigate the effects of hormonal shifts during aging.
What is insulin resistance and how is it related to estrogen and progestrone levels?
In insulin resistance, the cells’ response to insulin becomes impaired, leading to reduced glucose uptake and utilization. As a result, the body’s blood sugar levels remain elevated, leading to a condition known as hyperglycemia. To compensate for the decreased sensitivity of cells to insulin, the pancreas may produce even more insulin, leading to hyperinsulinemia (elevated insulin levels).
The relationship between insulin resistance and estrogen and progesterone levels in women is complex and can be influenced by various factors:
- Estrogen: Estrogen has been shown to enhance insulin sensitivity, meaning that it helps the body’s cells respond more effectively to insulin’s actions. It promotes glucose uptake in the cells and may have a protective effect against insulin resistance. Women generally have higher insulin sensitivity than men, partly due to the presence of estrogen. However, during specific hormonal changes, such as the luteal phase of the menstrual cycle or menopause, when estrogen levels fluctuate, insulin sensitivity can vary.
- Progesterone: The relationship between progesterone and insulin sensitivity is not as well understood as that of estrogen. Some studies suggest that progesterone may have mixed effects on insulin sensitivity, depending on the context. For example, during the luteal phase of the menstrual cycle, progesterone levels rise, and some women may experience increased insulin resistance during this phase. However, more research is needed to fully understand progesterone’s role in insulin sensitivity.
- Menopause: As women approach and go through menopause, there is a decline in estrogen levels. Reduced estrogen levels have been associated with increased insulin resistance, potentially contributing to the higher risk of type 2 diabetes and weight gain observed in some postmenopausal women.
- Hormonal Birth Control: Some forms of hormonal birth control can also affect insulin sensitivity. For example, certain oral contraceptives may influence insulin sensitivity differently based on the type and dosage of hormones used.
It’s important to note that the relationship between hormones and insulin resistance can vary among individuals, and other factors such as genetics, lifestyle, and overall health also play a role. Women with concerns about insulin resistance or its relation to their hormonal status should consult with a healthcare professional for personalized evaluation and guidance. Maintaining a healthy lifestyle, including regular exercise and a balanced diet, can help improve insulin sensitivity and overall metabolic health.
What is a decrease in lipid removal for menopausal females?
During menopause, there is a decline in the production of female sex hormones, particularly estrogen and progesterone. Estrogen, in particular, plays a significant role in regulating lipid metabolism in women. It helps maintain healthy levels of high-density lipoprotein (HDL) cholesterol, often referred to as “good cholesterol,” and reduces low-density lipoprotein (LDL) cholesterol, known as “bad cholesterol.” Estrogen also has a positive impact on triglyceride levels, which are another type of blood lipid.
As estrogen levels decrease during menopause, the favorable effects it had on lipid metabolism may be diminished.
This can lead to several changes in lipid profiles:
- Increase in LDL Cholesterol: With declining estrogen levels, there may be a rise in LDL cholesterol levels, which can increase the risk of atherosclerosis (the buildup of plaque in arteries) and cardiovascular disease.
- Decrease in HDL Cholesterol: Estrogen helps maintain higher levels of HDL cholesterol, which is beneficial for heart health. However, during menopause, HDL cholesterol levels may decrease.
- Changes in Triglyceride Levels: Triglyceride levels may increase in some menopausal women due to hormonal changes, diet, and other factors.
These alterations in lipid profiles can contribute to an increased risk of cardiovascular disease and other metabolic complications in some menopausal females. Heart disease risk tends to rise after menopause, making lipid management and cardiovascular health especially important during this life stage.
What is the estrogen receptor alpha?
When estrogen, a female sex hormone, binds to its receptor (ERα or ERβ) within the cell, it initiates a series of cellular responses, influencing gene expression and various physiological processes. These processes are collectively referred to as estrogen signaling.
Specifically, estrogen receptor alpha (ERα) is predominantly expressed in the female reproductive organs, such as the uterus and mammary glands. It plays a significant role in regulating the development and function of these tissues. ERα also has important effects on bone health, cardiovascular health, and the central nervous system.
Key functions of estrogen receptor alpha (ERα) include:
- Regulation of Gene Expression: When estrogen binds to ERα, it activates the receptor, which then binds to specific regions of DNA, called estrogen response elements (EREs), in the cell’s nucleus. This binding leads to the activation or repression of various genes, influencing the production of proteins involved in cell growth, tissue development, and other physiological processes.
- Promotion of Female Reproductive Health: ERα is crucial for the development and maintenance of the female reproductive system. It helps regulate the menstrual cycle, promotes the growth and differentiation of the uterine lining during the menstrual cycle, and supports mammary gland development during pregnancy and lactation.
- Bone Health: ERα signaling plays a protective role in bone health. Estrogen binding to ERα helps maintain bone density and inhibit bone resorption, reducing the risk of osteoporosis.
- Cardiovascular Effects: Estrogen signaling through ERα has vasoprotective effects on blood vessels, helping to maintain vascular function and reduce the risk of cardiovascular diseases in premenopausal women.
- Brain Function: ERα is also expressed in the brain, where it is involved in various aspects of cognitive function and neuroprotection.
The balance between ERα and ERβ and their specific actions in different tissues is crucial for maintaining overall health and hormone homeostasis. Dysregulation of estrogen signaling, either through abnormal receptor function or changes in estrogen levels, can contribute to various health issues, including hormone-related cancers, reproductive disorders, and metabolic conditions.
How can we improve our estrogen receptors post menopause?
- Hormone Replacement Therapy (HRT): Hormone replacement therapy involves the use of estrogen and sometimes progesterone to supplement the declining hormone levels in menopausal women. HRT can help alleviate menopausal symptoms and may have positive effects on estrogen receptor function. However, HRT should be discussed with a healthcare professional, as it comes with potential risks and benefits that vary among individuals.
- Regular Exercise: Engaging in regular physical activity, including both aerobic exercises and strength training, can have positive effects on estrogen receptors and overall health. Exercise has been shown to improve insulin sensitivity, bone health, and cardiovascular function in postmenopausal women.
- Healthy Diet: Adopting a balanced and nutrient-rich diet can support hormone health and overall well-being. Include plenty of fruits, vegetables, whole grains, lean proteins, and healthy fats in your diet. Phytoestrogens, found in certain plant foods like soy and flaxseeds, may have mild estrogen-like effects and could support estrogen receptor function.
- Weight Management: Maintaining a healthy weight is important for estrogen receptor function and overall health. Excess body fat, especially around the waist, can lead to increased inflammation and insulin resistance, negatively affecting hormone balance.
- Reduce Alcohol and Tobacco Use: Limit alcohol consumption and avoid tobacco use, as both can have negative effects on estrogen receptors and increase the risk of certain health issues.
- Stress Management: Chronic stress can impact hormone balance and overall health. Engage in stress-reducing activities such as meditation, yoga, deep breathing exercises, or spending time in nature.
- Bone-Healthy Nutrients: Adequate intake of calcium, vitamin D, and other bone-supporting nutrients can help maintain bone health during and after menopause.
- Regular Health Check-ups: Schedule regular check-ups with your healthcare provider to monitor hormone levels and overall health. Discuss any concerns or symptoms you may be experiencing.
How does progesterone levels impact uptake of insulin into the cell?
The impact of progesterone on insulin sensitivity and glucose uptake may vary depending on the context and other hormonal factors. Here are some ways in which progesterone levels can potentially affect insulin action:
- Progesterone and Insulin Sensitivity: Some studies suggest that progesterone may have mixed effects on insulin sensitivity. During certain phases of the menstrual cycle, particularly the luteal phase when progesterone levels are higher, some women may experience a temporary decrease in insulin sensitivity. This could lead to reduced glucose uptake by the cells and potentially higher blood sugar levels.
- Pregnancy: During pregnancy, progesterone levels are significantly elevated. Progesterone plays a crucial role in supporting pregnancy, but it can also lead to a state of relative insulin resistance in the body. This insulin resistance ensures that sufficient nutrients are available to support fetal growth and development.
- Hormonal Balance: The balance between progesterone and other hormones, particularly estrogen, also plays a role in insulin sensitivity. Progesterone’s effects on insulin action may be influenced by the overall hormonal environment in the body.
- Interaction with Estrogen: Progesterone can interact with estrogen, and the balance between these hormones can impact insulin sensitivity. For example, some studies suggest that the combination of progesterone and estrogen in certain forms of hormonal birth control may lead to increased insulin resistance.
It is essential to note that the effects of progesterone on insulin sensitivity can vary among individuals and may depend on factors such as genetics, lifestyle, and overall health. Moreover, progesterone’s impact on insulin sensitivity is generally considered to be less significant than that of other hormones like estrogen.
How does estrogen and progesterone play a role in glucose metabolism and glucose homeostasis?
1. Estrogen and Glucose Metabolism:
- Enhanced Insulin Sensitivity: Estrogen has been shown to improve insulin sensitivity, meaning that it helps the body’s cells respond more effectively to insulin. Insulin is a hormone that facilitates the uptake of glucose from the bloodstream into cells, where it can be used for energy. Increased insulin sensitivity allows cells to take up glucose more efficiently, which helps maintain normal blood sugar levels.
- Inhibition of Gluconeogenesis: Gluconeogenesis is the process by which the liver produces glucose from non-carbohydrate sources, such as amino acids and fatty acids. Estrogen has been found to suppress gluconeogenesis, preventing excess glucose production in the liver and aiding glucose regulation.
- Support for Beta Cell Function: Beta cells in the pancreas produce and release insulin. Estrogen may support beta cell function, promoting optimal insulin secretion in response to changes in blood glucose levels.
2. Progesterone and Glucose Metabolism:
- Regulation of Insulin Release: Progesterone can influence insulin secretion from the pancreas. During the luteal phase of the menstrual cycle (after ovulation), when progesterone levels rise, some women may experience a mild reduction in insulin sensitivity, leading to a slight decrease in glucose tolerance.
3. Hormonal Interplay:
- Menstrual Cycle: Throughout the menstrual cycle, estrogen and progesterone levels fluctuate, influencing glucose metabolism differently during different phases. For instance, estrogen dominance during the follicular phase (before ovulation) may enhance insulin sensitivity, while progesterone’s effects during the luteal phase may lead to a slight reduction in insulin sensitivity.
- Pregnancy: During pregnancy, progesterone levels increase significantly, creating a state of relative insulin resistance in the body. This helps ensure an adequate supply of nutrients to support fetal growth and development. The body adapts to this by increasing insulin secretion to meet the increased demand for glucose utilization.
It is important to recognize that estrogen and progesterone’s effects on glucose metabolism can be influenced by various factors, including the balance between these hormones, individual hormone levels, lifestyle choices, and overall health status. Moreover, these hormonal effects may differ among women and can be influenced by genetic variations.
Overall, the interplay between estrogen and progesterone in glucose metabolism and glucose homeostasis is complex and is an active area of ongoing research. The balance between these hormones, as well as their interactions with other hormones and cellular pathways, helps to maintain blood sugar levels within a healthy range and supports overall metabolic health.
How does the loss of progesterone relate to loss of Growth Hormone and IGF-1
- Progesterone and Growth Hormone (GH):
- Some animal studies have indicated that progesterone may have inhibitory effects on growth hormone secretion. These studies have shown that high levels of progesterone can reduce GH release from the pituitary gland, which could affect overall growth and metabolism.
- In humans, evidence on the direct relationship between progesterone and GH is limited, and the potential impact of progesterone on GH secretion is not well-established.
- Progesterone and Insulin-Like Growth Factor 1 (IGF-1):
- IGF-1 is a hormone produced primarily in the liver in response to GH stimulation. It plays a crucial role in growth and tissue repair.
- Progesterone has been shown to influence IGF-1 levels in some studies. For example, during pregnancy, when progesterone levels are high, IGF-1 levels tend to rise as well to support fetal growth and development.
- Additionally, some research suggests that progesterone may enhance the actions of IGF-1, particularly in promoting breast tissue development during pregnancy.
It’s important to note that hormones in the body often interact with one another in complex ways, and the balance of these interactions c an vary significantly based on individual differences, hormone levels, and physiological context.
an vary significantly based on individual differences, hormone levels, and physiological context.
The loss of progesterone typically occurs during menopause when the ovaries stop producing significant amounts of sex hormones, including estrogen and progesterone. Menopause can also lead to changes in GH and IGF-1 levels, as hormonal imbalances and shifts occur.
While menopause itself can impact hormone levels, including GH and IGF-1, the specific relationship between the loss of progesterone and the decline of GH and IGF-1 remains an area of ongoing research. It is crucial to consider multiple factors influencing hormone levels and their interactions when studying the effects of hormonal changes on the body’s physiology. Further research is needed to fully understand the complex relationships among these hormones.
How does progesterone levels impact our insulin sensitivity?
- Luteal Phase of Menstrual Cycle: During the luteal phase of the menstrual cycle, which occurs after ovulation, progesterone levels rise while estrogen levels decline. Some women may experience a temporary decrease in insulin sensitivity during this phase. This decrease in insulin sensitivity is thought to be a normal physiological adaptation that helps ensure adequate nutrient availability for potential pregnancy. However, the impact on insulin sensitivity during this phase is generally mild and transient.
- Pregnancy: During pregnancy, progesterone levels increase significantly to support fetal growth and development. Progesterone, along with other hormones produced during pregnancy, can lead to a state of relative insulin resistance. This insulin resistance ensures that sufficient nutrients, including glucose, are available to support fetal growth and development. The body compensates for the reduced insulin sensitivity by increasing insulin secretion to meet the increased demand for glucose utilization.
- Hormonal Interplay: The balance between progesterone and other hormones, such as estrogen, can also influence insulin sensitivity. For example, estrogen has been shown to enhance insulin sensitivity, and its interplay with progesterone can impact the overall effects on insulin action.
It’s important to note that the effects of progesterone on insulin sensitivity may vary among individuals and can be influenced by other factors, such as genetics, lifestyle, and overall health. Moreover, progesterone’s impact on insulin sensitivity is generally considered to be less significant than that of other hormones like estrogen.
Progesterone’s effects on insulin sensitivity are part of the body’s complex hormonal regulatory system. While the interactions between hormones and insulin sensitivity are essential for maintaining glucose homeostasis, they can also be influenced by various physiological and environmental factors.
Estrogen levels can have significant effects on insulin sensitivity and fat metabolism in muscle cells. Estrogen is a female sex hormone that plays a crucial role in various physiological processes, including glucose and lipid metabolism.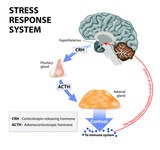
1. Insulin Sensitivity:
- Enhanced Insulin Sensitivity: Estrogen has been shown to enhance insulin sensitivity in various tissues, including muscle cells. When estrogen binds to its receptors in the cell, it can stimulate signaling pathways that improve the cell’s response to insulin. Enhanced insulin sensitivity allows muscle cells to take up glucose more effectively from the bloodstream, promoting better glucose utilization for energy and reducing blood sugar levels.
- Regulation of Glucose Transporters: Estrogen can influence the expression and activity of glucose transporters, such as GLUT4, in muscle cells. These transporters play a key role in facilitating the entry of glucose into the cell. Estrogen’s effect on glucose transporters contributes to its role in enhancing insulin sensitivity.
2. Fat Metabolism in Muscle Cells:
- Increased Fat Oxidation: Estrogen has been shown to increase the oxidation (burning) of fatty acids in muscle cells. This means that muscle cells are more efficient in using fat as an energy source during exercise and other metabolic activities. This effect can help spare glucose utilization, contributing to better glucose availability for other tissues.
- Regulation of Lipid Metabolism Enzymes: Estrogen can modulate the expression and activity of various enzymes involved in lipid metabolism in muscle cells. For example, estrogen may increase the activity of enzymes responsible for fatty acid oxidation and reduce the activity of enzymes involved in fat storage.
- Lipoprotein Lipase (LPL) Activity: Estrogen can also influence lipoprotein lipase (LPL) activity in muscle cells. LPL is an enzyme that plays a role in the breakdown of triglycerides in lipoproteins (such as chylomicrons and VLDL) to release fatty acids for cellular uptake. Estrogen’s effects on LPL activity can impact the availability of fatty acids for energy use in muscle cells.
It’s important to note that the effects of estrogen on insulin sensitivity and fat metabolism can vary among individuals and may depend on factors such as genetics, hormone levels, and overall health. Additionally, the impact of estrogen can be influenced by other hormones and factors present in the body’s hormonal milieu.
Overall, estrogen’s role in insulin sensitivity and fat metabolism in muscle cells highlights its significance in maintaining metabolic health and potentially reducing the risk of metabolic disorders, such as insulin resistance and type 2 diabetes.
Estrogen receptors (ERs) are found throughout the body, and their distribution varies among different tissues. Estrogen receptors are proteins located inside the cells that act as targets for the hormone estrogen. When estrogen binds to these receptors, it initiates a series of cellular responses and influences gene expression, leading to various physiological effects.
- Estrogen Receptor Sites in the Body:
- Breast Tissue: Estrogen receptors are abundant in breast tissue, where estrogen plays a crucial role in the development and function of the mammary glands.
- Uterus: The uterus contains estrogen receptors, and estrogen signaling is essential for regulating the menstrual cycle and preparing the uterine lining for potential pregnancy.
- Ovaries: Estrogen receptors are present in the ovaries, where estrogen helps control the development and release of eggs during the menstrual cycle.
- Brain: The brain also contains estrogen receptors, and estrogen influences various aspects of brain function, including mood, cognition, and memory.
- Bones: Estrogen receptors are found in bone cells, and estrogen plays a vital role in maintaining bone density and bone health.
- Cardiovascular System: Estrogen receptors are present in blood vessel walls and various cardiovascular tissues. Estrogen has vasoprotective effects and may help maintain vascular health in premenopausal women.
- Liver: The liver contains estrogen receptors, and estrogen influences various liver functions, including lipid metabolism.
- Production of Estrogen:
- Ovaries: Before menopause, the ovaries are the primary source of estrogen production in women. The ovaries produce estrogen, mainly estradiol (E2) and some estrone (E1), during the menstrual cycle. Estrogens are responsible for regulating the menstrual cycle, promoting ovulation, and maintaining female reproductive health.
- Adrenal Glands: The adrenal glands, located on top of each kidney, also produce small amounts of estrogens, including E2 and E1, especially after menopause when ovarian estrogen production declines. Adrenal androgens, such as DHEA and androstenedione, can be converted into estrogens in peripheral tissues like fat cells through a process called aromatization.
During menopause, when ovarian estrogen production decreases significantly, the adrenal glands and peripheral tissues become more important sources of estrogen production. This peripheral production of estrogen from androgens can help maintain some estrogen levels in the body, albeit at lower levels compared to premenopausal women.
The presence of estrogen receptors throughout the body allows estrogen to exert its diverse effects on various physiological processes, making it a crucial hormone in maintaining overall health and well-being in both men and women.

What are you doing today to manage your chronic stress load?